.png)
Standards of Care for Suspected and Confirmed Compressive Cauda Equina Syndrome
Background
Cauda Equina Syndrome (CES) is a relatively rare, but very disabling condition. It causes misery to affected patients that is reflected in the cost of managing the disability and litigation which results from it. It is possible that a proportion of established CES MAYBE avoidable with appropriate and timely management. We have produced these guidelines in order to try and improve the care for patients with this condition.
Definitions
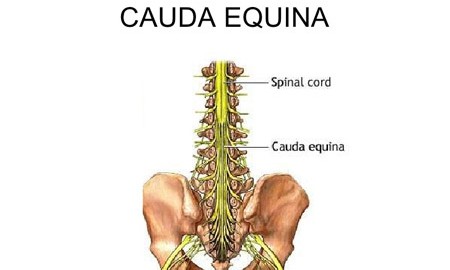
A patient presenting with acute (de-novo or as an exacerbation of pre-existing symptoms) back pain and/or leg pain, with a suggestion of a disturbance of their bladder or bowel function and/or saddle sensory disturbance, should be suspected of having a cauda equina syndrome. Most of these patients will not have critical compression of the cauda equina. However, in the absence of reliably predictive symptoms and signs, there should be a low threshold for investigation with an EMERGENCY scan. The reasons for not requesting a scan should be clearly documented.
Imaging
The appropriate investigation of these patients is an MRI scan except where specifically contraindicated. The investigation should be undertaken as an emergency. It is very difficult to justify waiting until the end of an elective MRI list. The spinal societies (BASS and SBNS) strongly recommend that MRI scanning should be undertaken urgently at the hospital receiving the patient in order to ensure timely diagnosis and, when appropriate, immediate referral and transfer to a spinal unit.
There are four potential outcomes from the investigation:
- Cauda equina compression confirmed. This should precipitate an urgent referral to the appropriate surgical service.
- Cauda equina compression excluded, but a potential structural explanation of pain identified. This should precipitate appropriate advice that may include referral to the appropriate surgical service.
- Non-compressive pathology may be identified (for example, demyelination) which should precipitate referral to the appropriate service.
- No explanation of the patient’s symptoms may be apparent. In these circumstances an appropriate plan for further management is required.
Surgery
Nothing is to be gained by delaying surgery and potentially much to be lost. Decompressive surgery should be undertaken at the earliest opportunity, taking into consideration the duration of pre-existing symptoms and the potential for increased morbidity whilst operating in the small hours. We recommend reasons for any delay in surgery be documented.
Counselling
All patients undergoing surgery for CES should be counselled that the aim of surgery is to preserve that function present at the time of surgery. There is scope for improvement, but there is a small risk of making matters worse including paralysis of the legs, complete loss of bladder and bowel control and impotence/sexual dysfunction.
Does Early Surgical Decompression in Cauda Equina Syndrome Improve Bladder Outcome?